Practicing radioactive therapy. Before a single patient.
I led the design of the Mobile RLT Institute — the VR experience within Novartis's Radioligand Therapy program — from storyboarding through dev handoff. Two phases, four clinical spaces, 148+ storyboard frames.
Role
VR Design Lead
Timeline
May 2025 – 2026
Team
Real Chemistry + Novartis Medical Affairs
Platform
VR (Meta Quest)
Summary
Launched at ASTRO 2025 — recognized by the Novartis CEO at Meet the Management London.
A VR training experience for radioligand therapy — the radioactive drug protocols HCPs used to learn only on real patients. One interaction language built in Phase 1, scaled across 4 clinical spaces over 18 months. 148+ storyboard frames shipped.
Problem
HCPs administering radioligand therapy — radioactive drugs — had no safe place to practice complex protocols before treating a real patient.
My role
Led VR experience design from storyboarding through dev handoff. Built the interaction pattern in Phase 1, scaled it across 4 clinical spaces.
Team + Timeline
Real Chemistry + Novartis Medical Affairs · May 2025–2026 · VR (Meta Quest)
The Mobile Novartis RLT Institute · ASTRO 2025 attract loop · provider/magnified view toggle, guided demonstrations from real clinics
The setup
Radioligand therapy is too dangerous to learn by doing.
RLT is a targeted cancer therapy using radioactive pharmaceuticals. Training on live patients isn't an option. Goal: take the headset off knowing "I can do it and I can do it safely."
Where this fits in the broader program ↓
The immersive complement to Novartis's web-based Virtual RLT Institute (a separate Real Chemistry workstream). Audience: community oncologists, radiation oncologists, urologists, nurses, nuc-med techs, radiation therapists. Products: LUTATHERA (neuroendocrine tumors) and PLUVICTO (metastatic prostate cancer). Part of Novartis's Project Breakthrough initiative.
4 Spaces
Simulated in VR
Hot Lab, Treatment Room, Decay Space, patient Bathroom — each with unique protocols
148+
Storyboard frames designed
Frame-by-frame interaction specs before any 3D production began
2 Phases
May → Oct 2025
Phase 1 established the system; Phase 3 proved it scales
Treatment Room — Gravity method Step 1 in the magnified view, with the Magnified/Provider toggle floating in the spatial environment
Spatial design meets clinical protocol.
Established VR principles weren't built for regulated pharma training with low-VR-literacy clinicians, exact-protocol fidelity, and tight file-size budgets.
Constraint
Low VR literacy, high-stakes content
Laser-pointer input over gesture controls. Oversized UI targets. Voiceover guides because you can't predict where users are looking.
Decision
Process- vs. location-based navigation?
Final answer was hybrid: a home diorama for room selection, then a guided flow within each room ending in "where do you want to go next?"
What this VR actually is (180° live-action + 3D hybrid) ↓
Not fully CGI — a hybrid built for realism within file-size constraints:
180° live-action video filmed in real clinical environments, with stepwise interactivity on top
"Standard cam" inset footage for zoomed-in detail-oriented actions
180° photos and illustrations with interactive hotspots where live action wasn't required
3D model of an idealized facility as the navigation hub — the only "fully built" 3D layer
My interaction work was mostly overlaying UI affordances on real footage — not designing 3D environments from scratch.
Layout 1 — Module-based with nested panels. A 4-item icon checklist card sits beside an Expert Insight side card. Linear, scannable, content-dense.
Layout 2 — Linear toolbar. Content card up top, controls bar at the bottom. The math formula gets its own card; the scrubber is always within thumb reach.
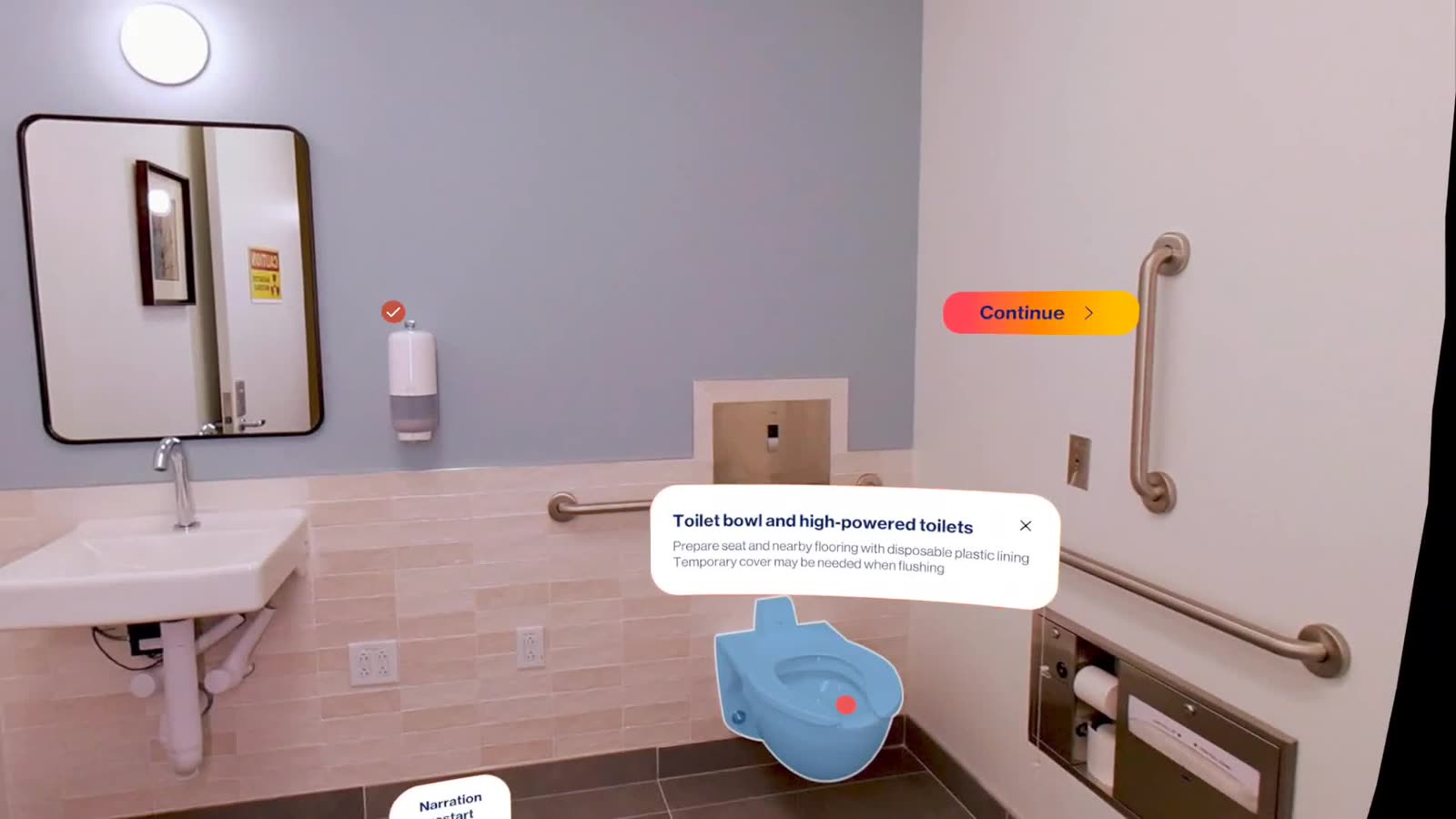
Layout 3 — Spatial popups. Panels float in the room, anchored to the live 180° scene. Back + Narration restart hover in the periphery, not inside the panel.
Three layout directions explored with the client. The shipping system kept the spatial panel from Layout 3 and absorbed pieces of Layouts 1 and 2 wherever they were a better fit.
Process
148 frames before a single 3D model.
Every VR interaction was designed as a numbered storyboard frame — so clinicians could approve interactions on paper before expensive 3D production began.
What I owned
VR interaction architecture
Storyboard system (148+ frames)
Phase 1 + Phase 3 design lead
Client presentations (5+ rounds)
Dev handoff specs
What I built on
Real Chemistry agency team (UX, UI, project, account)
Novartis Medical Affairs (clinical SMEs)
Virtual RLT Institute as content authority
Novartis brand system + design tokens
What I didn't own
3D production / Unity build (production team)
Storyboard illustration (art team)
Virtual RLT Institute web platform (separate workstream)
AI in this project: a narrow role. Claude translated multi-page RLT protocols into voiceover scripts and frame-level beats — "what do you see, what can you do, what happens next" — before the illustrator drew each frame. The rest was hand-built.
The storyboard methodology in production — a 3-card educational intro panel reused at the start of every chapter, voiceover-synced and with a single Continue CTA
Chapter navigation drilldown — the 000.0–012.x numbering route surfaced as breadcrumbs
Inline references panel — NRC, AAPM, and journal citations surface inside the VR, with the Novartis isi footer
Build, then scale
Phase 1 set the patterns. Phase 3 stress-tested them.
Build the interaction language once on the Treatment Room and Bathroom. Prove it scales on the Hot Lab — 6 procedures and 115 frames, more branching and more safety-critical decisions than anything before.
Phase 1 · Treatment Room + Bathroom
Tx Room
The syringe administration method
Two variants — manual (with shield) and with pump — as distinct VR sequences. Magnified/provider toggle mid-procedure.
Bathroom
Prep, cleanup, and scenarios
Real-environment imagery with interactive hotspots, side panels with audio, and before/after toggles.
System
Equipment glossary + navigation
Intro animation, home diorama, equipment glossary — supporting systems that made the core procedures learnable.
Treatment Room — Syringe pump method Step 3 in motion: the OFF-to-IV flow-direction diagram floats beside the magnified live-action procedure
Bathroom with VR hotspots, navigation hub, and state toggle
Expert Insight card in motion — the layered card system overlaid on a live 180° scene
Phase 3 · Hot Lab + Decay Space
Adaptation
Spill cleanup as reusable module
Built as a modular component that drops into any room with location-specific guidance — first test of the Phase 1 system's flexibility.
New ground
Package check-in
Entirely new procedure with no Phase 1 precedent. Used the established hotspot-plus-panel pattern with sequential step tracking.
Scaling
Decay Space
Simpler room (33 frames) but needed new UI for time-based information. Phase 1 patterns stretched without breaking.
Decay Space in motion — CLOSED/OPEN waste-bin educational panel introducing the half-life decay rule (≤120 days), with active hotspots waiting for selection
Hot Lab — Package check-in Step 2 in motion: a procedure with no Phase 1 precedent, built on the established step-tracking pattern
Pattern System
Five patterns. Built once. Reused everywhere.
When Phase 3 doubled the room count, none of these had to be redesigned — they stretched.
01 · Interaction
Hotspot + side panel
Tap a hotspot → side panel with description, audio, and visual. One component drove bathroom prep, equipment learning, and Hot Lab procedures.
02 · Pacing
Voiceover-guided chapters
Passive viewing → knowledge check → gamified moment. Voiceover guides users because you can't predict where they're looking. One pacing structure, every chapter.
03 · Comparison
State toggle
One A/B switch, three uses: standard vs. prepared bathroom, magnified vs. provider perspective, clean vs. contaminated in spill cleanup.
04 · Reuse
Modular drop-in scenario
Spill cleanup as a self-contained component that drops into any room with location-specific guidance — the proof the Phase 1 system was modular.
05 · System
Equipment glossary
Grid of every instrument with on-tap detail and clinical-accurate descriptions. Built once — drives equipment learning across all four spaces.
Impact
What we shipped, where it landed
A full VR simulation across four clinical spaces, launched on the world's largest radiation oncology stage and a Novartis investor meeting in the same year.
ASTRO 2025
Phase 1 launch
American Society for Radiation Oncology Annual Meeting — the field's flagship congress
London
Meet Novartis Management
Novartis investor meeting — the CEO came by the booth to recognize the team
8 congresses
2025 RLT Institute presence
Strategic Novartis events with creative installations · 9 chapters live, 11 more in the 2026 pipeline
From workshop to field rollout
May 2025
Workshop
MVP scope and the laser-pointer-over-gesture decision.
Oct 2025
Dev handoff + ASTRO launch
Frame-by-frame specs to the Unity team. Live on the ASTRO floor.
2026
Build + RTS field rollout
Edge-case iteration and rollout to the Radioligand Therapy Specialist field team.
Market position
Post-ASCO 2025 market research confirmed Novartis is perceived as a leader in RLT.
"The team's ability to anticipate challenges, navigate complexity, present clear options, and deliver well-considered creative solutions has been greatly appreciated. The RLT Institute is playing a meaningful role in operational readiness and education across the field."
"The VR content is impressive enough that clinics want to buy VR headsets to have the content on hand all the time."
Reflection
What I'll carry forward
Storyboards are the prototype
In VR, you can't click through a Figma file. Storyboards became the review artifact that unlocked clinical sign-off before expensive 3D production.
Regulated domains demand translation, not simplification
Clinical protocols are complex for a reason. The job was making them learnable without making them inaccurate — every shortcut validated with stakeholders.
Spatial design is spatial writing
Every VR frame is a sentence: what do you see, what can you do, what happens next. Numbered frames kept designers, clinicians, and developers reading the same story.